 TRIP COST
TRIP COSTACE trips are for teams of 15 or more, but individuals and teams smaller than 15 can be accommodated in certain circumstances.
Length: 8 days/7 nights (standard trip is Saturday to Saturday)
Cost per person: $850 + airfare (including $100 non-refundable deposit)
Please note starting January 1, 2025, the trip cost per person will be $899 + airfare (including $100 non-refundable deposit).
Children 12 and under are half price. Children 3 and under are free.
We require that our teams arrive and depart from Sangster/Montego Bay airport (MBJ), arriving prior to 3:00 pm (2:00 pm is better) and departing no earlier than 1:00 pm. It’s approximately a 2.5 hour drive to the hotel. Another airport option is Ian Fleming International Airport (OCJ), which has limited airline/flights but is 20 minutes from the hotel. We have no time requirements for pick-up and drop-off at OCJ, though there may be a wait time for afternoon hotel check-in.
What is included in the cost?
√ Ground transportation between airport and hotel (2 hour trip each way)
√ Room and Board (group price based on 4-6 people per room)
√ All meals during your stay at the hotel
√ 24-hour security
√ Daily bus transportation to local outreach (10-35 minutes)
√ Most construction supplies, if applicable (paint, block, cement, etc.)
√ All tips and taxes
√ Full local staff and ACE staff
√ Access to hotel pool, tuck shop, and ocean side fire pit
√ Optional site trip for one leader to Jamaica prior to trip (airfare not included – please inquire about dates)
√ A life-changing experience!
X Airfare costs – flight requirements above must be met for free ground transportation, with arrival and departure on Saturdays (unless arrangements are made prior to booking)
X Mandatory short-term travel insurance. We can coordinate this through our ACE partner, Travel Team Brokers (contact us for pricing) Or teams can provide their own (proof of insurance required).
X Food during travel to and from the airport
X Off-day costs (an afternoon activity planned by ACE with transportation; bring $35 to cover lunch and admission expenses)
X Optional purchases at hotel or at off-day site
 UPCOMING MEDICAL TRIP DATES:
UPCOMING MEDICAL TRIP DATES:By partnering with medical groups from the US, ACE holds quarterly medical clinics throughout the parish. In working with the Jamaican Ministry of Health, our teams are able to make regular visits to the government clinics, enabling these communities to receive the care and treatment they so desperately need. By holding regular clinics, the health problems of the communities are treated regularly therefore decreasing the acuteness of the illnesses.
Our trips run Saturday to Saturday and the cost is $850 per person for the entire week; Please note starting January 1, 2025, this price goes up to $899 per person. This includes your stay and food at Galina Breeze Hotel, transportation to and from the airport, organized medical clinics, 24-hour security, and transportation to and from the clinic sites. (Free day activity is an additional $35 that you will need to have with you on the island) Airfare is not included. Please note that this is a group rate and is based on 4-6 per room. If you need a private room and there is availability (determined by ACE and the hotel), you may have one for an additional $25/night for double occupancy, $50 for single occupancy.
If you’re interested in learning more about our medical trips, or you wish to book a trip, click the button below to contact our stateside office.
 About the Scriptures
About the Scriptures
We believe the entire Bible is the inspired Word of God and that men were moved by the Spirit of God to write the very words of Scripture. Therefore, we believe the Bible is without error.
About God
We believe in one God who exists in three distinct persons: Father, Son, and Holy Spirit. We believe that Jesus Christ is the second member of the Trinity and (the Son of God) who became flesh to reveal God to humanity and to become the Savior of the lost world.
About Humanity
We believe that all people were created in the image of God to have fellowship with him but became alienated in that relationship through sinful disobedience. As a result, people are incapable of regaining a right relationship with God through their own efforts.
About Salvation
We believe that the blood of Jesus Christ, shed on the cross, provides the sole basis for the forgiveness of sin. Therefore, God freely offers salvation to those who place their faith in the death and resurrection of Christ as sufficient payment for their sin.
About the Christian Life
We believe all Christians should live for Christ and not for themselves. By obedience to the Word of God and daily yielding to the Spirit of God, every believer should mature and be conformed to the image of Christ.
Agenda items may include
There will be an “off-day” opportunity, usually a beach or other relaxing activity, toward the end of your week; teams must bring $35 per person in cash to participate. This is a perfect way to end a week of hard work!
 The negative impact of poverty is most deeply felt by the youngest and most vulnerable part of the community—the children. Like Jesus in Matthew 19, ACE believes it is our duty to welcome these children with open arms, offering them love and protection. We are committed to give the children of our community a chance to break out of the cycle of poverty by empowering them to reach their full potential by being educated, cared for, and in good health.
The negative impact of poverty is most deeply felt by the youngest and most vulnerable part of the community—the children. Like Jesus in Matthew 19, ACE believes it is our duty to welcome these children with open arms, offering them love and protection. We are committed to give the children of our community a chance to break out of the cycle of poverty by empowering them to reach their full potential by being educated, cared for, and in good health.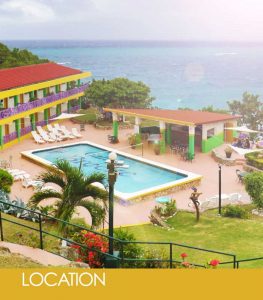

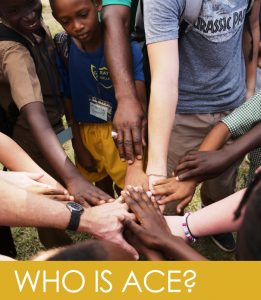 WE ARE a Christ-based outreach ministry dedicated to community transformation in the parish of St.Mary, Jamaica through strategic initiatives in education, enterprise, healthcare, and discipleship.
WE ARE a Christ-based outreach ministry dedicated to community transformation in the parish of St.Mary, Jamaica through strategic initiatives in education, enterprise, healthcare, and discipleship.
HOW DO WE DO IT? ACE enables volunteers to join in its outreach through a variety of hands-on experiences. Individuals and groups from all over the world come to volunteer their talents and know-how, which helps provide self-sustaining solutions to local problems, and in turn, empowers the people of St. Mary, Jamaica.
WHAT IS OUR IMPACT? With more than 30 years experience working in Jamaica and a deep understanding and passion for the country, ACE serves as a model for successful community outreach. Additionally, while making a direct impact during their time in Jamaica, volunteers often return home with a new understanding and passion for service which results in continued ministry to those in need throughout the globe.
 Being a beacon for Christ is the fundamental purpose of everything we do. Equally important is how we do it. Our duty is to let His light penetrate the darkness by being love in action.
Being a beacon for Christ is the fundamental purpose of everything we do. Equally important is how we do it. Our duty is to let His light penetrate the darkness by being love in action.
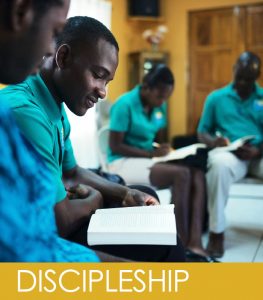
We don’t just talk the talk, we walk the walk… because faith without action is dead. As we are often asked why we do what we do, the answer is simply, the door is open for us to lead the way for children and families to experience a relationship with their Saviour, so we are seizing the opportunity and partnering with Christ. We work with our local church to ensure continued spiritual growth and care.
Community Discipleship- Discipleship is intentionally incorporated into everything we do. In addition to one-on-one discipleship efforts, ACE coordinates and hosts conferences for more in depth mentoring and outreach to men, women, business people and couples.
 Marla Fitzwater, Founder and Executive Director of ACE, arrived on the island in 1988 coordinating short-term mission teams to work in Jamaica. Her work began to form what is now ACE.
Marla Fitzwater, Founder and Executive Director of ACE, arrived on the island in 1988 coordinating short-term mission teams to work in Jamaica. Her work began to form what is now ACE.
During the early years, Marla quickly observed that those receiving the primary benefit from volunteer efforts were actually the people and organizations who were serving. These visitors were touched by the experience and inspired to continue serving others upon returning home. Ironically, the local community had not experienced any long lasting change. Despite the projects and improvements, the community inevitably returned to a poverty state physically, mentally and most of all, spiritually. She also learned that poor healthcare and lack of education was a reality and that without improvements in those two basic areas, people just wouldn’t have a chance to grow and flourish the way God intended.
Through these tough lessons, the strategy for ACE’s outreach was born. To this day, our ministry focuses in four main areas of Impact: education, healthcare, enterprise, and discipleship.
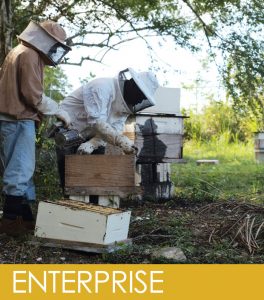 There is an old proverb, “If you give a man a fish, he’ll eat for a day, but if you teach a man to fish, he’ll eat for a lifetime.” History proves that lasting change in a poverty culture is achieved by empowering the people to reach their full potential and become self-sustaining. ACE is invested in our community long-term and in conjunction with our partners in the US, we are identifying the circumstances of those around us in order to find real solutions for their unique needs.
There is an old proverb, “If you give a man a fish, he’ll eat for a day, but if you teach a man to fish, he’ll eat for a lifetime.” History proves that lasting change in a poverty culture is achieved by empowering the people to reach their full potential and become self-sustaining. ACE is invested in our community long-term and in conjunction with our partners in the US, we are identifying the circumstances of those around us in order to find real solutions for their unique needs.
History proves that lasting change in a poverty culture is achieved by empowering the people to reach their full potential and become self-sustaining. ACE is invested in our community long-term and in conjunction with our partners in the US, we are identifying the circumstances of those around us in order to find real solutions for their unique needs.
 The ministry of Jesus on earth was teaching and healing. Rarely is there one without the other. We have found that if you talk about the love of God but fail to meet the basic and urgent needs of the people, it might as well be hypocrisy.
The ministry of Jesus on earth was teaching and healing. Rarely is there one without the other. We have found that if you talk about the love of God but fail to meet the basic and urgent needs of the people, it might as well be hypocrisy.
By partnering with medical groups from the US, ACE holds quarterly medical clinics throughout the parish. In working with the Jamaican Ministry of Health, our teams are able to make regular visits to the government clinics, enabling these communities to receive the care and treatment they so desperately need. By holding regular clinics, the health problems of the communities are treated regularly therefore decreasing the acuteness of the illnesses.